
Human pregnancy
The pregnancy or pregnancy (from «gravidus», and this from the Latin gravĭdus) is the period between implantation of the zygote in the uterus, until the time of delivery, in terms of the significant physiological, metabolic and even morphological changes that occur in women aimed at protecting, nourishing and allowing the development of the fetus, such as the interruption of menstrual cycles, or the increase in the size of the breasts to prepare for lactation. The term gestation refers to the physiological processes of growth and development of the fetus inside the maternal uterus. Strictly speaking, and well expressed, gestation refers to the development of the fetus and pregnancy refers to the changes in the woman that make it possible, although in practice many people use both terms as synonyms.
In humans, pregnancies are usually single, although multiple pregnancies can occur. The application of assisted reproductive techniques is increasing the incidence of multiple pregnancies in developing countries.
Human pregnancy lasts between 38 to 40 weeks from fertilization, approximately 9 months. Taking into account the variation that occurs in relation to the duration of pregnancy, it is more accurate to say that the duration of pregnancy usually lasts between 37 and 42 since only 4% of women give birth on the date predicted by the rule from Naegele. If the baby is born before 37 weeks it is considered a premature birth, and if it is born after 42 weeks it is considered a post-term birth.
The first trimester is the time of greatest risk of miscarriage; the beginning of the third trimester is considered the point of viability of the fetus, that is, the moment from which it can survive extrautero.
Definition and types

In 2007, the Committee on Ethical Aspects of Human Reproduction and Women's Health of the International Federation of Gynecology and Obstetrics (FIGO) defined pregnancy as the part of the human reproduction process that begins with the implantation of the conceptus in women.[citation required] Pregnancy begins at the time of nesting and ends with delivery. The legal definition of pregnancy follows the medical definition: for the World Health Organization (WHO) pregnancy begins when implantation ends, which is the process that begins when the blastocyst adheres to the wall of the uterus (about 4 or 6 days after fertilization). The blastocyst then breaks through the uterine endometrium and invades the stroma. The implantation process ends when the defect in the surface epithelium closes and the nesting process is completed, thus beginning the pregnancy. This occurs between days 12 to 16 after fertilization.
An ectopic pregnancy or extrauterine pregnancy is one that occurs outside the uterus, due to an abnormal implantation of the fertilized ovum (usually in one of the two fallopian tubes) and much less frequently in the cavity peritoneal (abdominal pregnancy) and other sites.
An unwanted pregnancy is one that occurs without the desire or prior planning on the part of the woman and in the absence or failure of adequate precoital contraceptive methods and the ineffectiveness or non-administration of contraceptive methods emergency after intercourse to prevent a possible pregnancy.
In the event of an unwanted pregnancy and in accordance with the principles of reproductive health of the WHO, the woman can continue with the pregnancy and carry the pregnancy to term, or practice a voluntary interruption of the pregnancy or abortion induced, either through a medical abortion or a surgical abortion, depending on the gestation period and always with adequate health care, taking into account that this practice may be illegal in some countries.
Globally, 38% of pregnancies are unwanted, 21% of them are in adolescents (of which between 30 and 60% end in abortion); about 80 million unwanted pregnancies each year out of a total of 210 million pregnancies worldwide.
General characteristics

Fertilization is produced by the union of the female gamete with the male gamete. There is some controversy about when the pregnancy begins, having different opinions about it.
For the World Health Organization (WHO), pregnancy begins when the implantation of the embryo in the uterus ends, since, in many cases, the egg is fertilized but does not implant itself and the pregnancy does not begin. Implantation is a process that begins about 5 or 6 days after fertilization and which consists of the adherence of the blastocyst to the wall of the uterus, when the blastocyst crosses the endometrium and invades the stroma, then the surface of the epithelium closes and becomes completes the nesting process, beginning then the pregnancy.
When it comes to in vitro fertilization, the embryo is fertilized in a test tube, it waits three days, and then it is transferred to the mother-to-be's uterus. At the time of nesting, pregnancy begins but, in most cases, the embryo does not attach and the female does not become pregnant.
For many scientists, life begins at the moment of fertilization and, therefore, pregnancy begins when a spermatozoon reaches and crosses the cell membrane of the ovum, fusing the nuclei and both sharing their genetic endowment to give rise to an egg cell or zygote, in a process called fertilization. Cellular multiplication of the zygote gives rise to the embryo, from whose development the adult individual derives.
The controversy about the moment in which pregnancy begins is not a minor fact since it affects ethical discussions in relation to abortion, assisted reproductive techniques and the use of contraceptives, which is why it remains very current.
Embryology is the part of medicine that studies the complex process of embryonic development from the moment of fertilization until the formation of the fetus, which is what the organism resulting from this development is called when childbirth has not yet taken place..
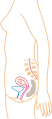
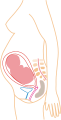
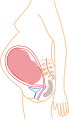
Inside the uterus, the fetus is floating in the amniotic fluid, and in turn the fluid and the fetus are encased in the amniotic sac, which is attached to the uterus. A thick mucus plug forms in the cervix during pregnancy to make it difficult for microorganisms to enter that cause intrauterine infection. This plug will be expelled during the onset of labor.
While it remains inside, the zygote, embryo or fetus obtains nutrients and oxygen and eliminates its metabolic wastes through the placenta. The placenta is anchored to the inner wall of the uterus and is attached to the fetus by the umbilical cord. The expulsion of the placenta after delivery is called labor.
Calendar
.gif)
According to its development, pregnancy is usually divided into three stages of three months each, with the aim of simplifying the reference to the different stages of development of the fetus.
During the first trimester the risk of miscarriage is greater (natural death of the embryo or fetus). This has a greater incidence in pregnancies achieved through in vitro fertilization, since the implanted embryo could stop developing due to failures in the chromosomes inherited from the gametes of its parents.
During the second trimester (from 14 weeks of gestation) the development of the fetus can begin to be monitored or diagnosed.
The third trimester marks the beginning of viability—approximately after the 25th week—meaning that the fetus could survive a premature birth, normal delivery, or cesarean section. Since from this moment the fetal lungs are almost fully formed, they just need to mature.
Expected date of delivery


Calculations to determine the probable date of delivery (PPD) are made using the date of the last menstrual period or by correlations that estimate gestational age using ultrasound. Most births occur between the 37th and 42nd week after the day of the last menstrual period, and only 5% of women give birth on the exact day of the probable date of delivery calculated by their health professional.
A study conducted at Brigham and Women's Hospital in Boston found that age, parity (number of children a woman has had), and ethnicity were the variables most correlated with length of pregnancy. Women who are multiparous (with more than one pregnancy), younger than 19 or older than 34, or African-American tend to have longer pregnancies than primiparous (first pregnancy), Caucasian women between the ages of 19 and 34. have found differences in the duration of pregnancy related to the height of the mother, with shorter women having shorter pregnancies on average.
Using the date of the last menstrual period, add seven days and subtract three months, giving the probable date of delivery. Thus, a safe date of last menstruation of November 28, 2017, will produce a probable date of delivery for September 5, 2018 —the year following the year of the last period is used. If the date of the last menstruation falls in the first two months, the current year is kept, in all other months, the subsequent year is used. Thus, a safe date of last menstruation of January 2, 2018, produces a probable date of delivery for October 9, 2018 —the year is maintained—
Detection and date of fertilization
The beginning of the pregnancy is detected with the presence of the hormone human chorionic gonadotropin (hCG) that is produced by the embryo after conception and later by the maternal plasma (the placenta), this hormone appears in the blood and in the urine of pregnant women up to 10 days after conception and this can be detected through urine and blood tests. Both types of test can only detect whether or not the woman is pregnant, but not the start date of the pregnancy.
Presumptive signs of pregnancy
Perhaps the first presumptive sign of pregnancy is amenorrhea, or the absence of a menstrual period. Because amenorrhea can occur from causes other than pregnancy, it is not always a safe start to pregnancy, especially if the woman does not have regular cycles. However, there may be several more signs that, together with amenorrhea, suggest pregnancy, such as: hypersensitivity in the nipples, dizziness, morning vomiting, drowsiness, alteration in the perception of odors, and intense desires for certain types of food (cravings). You can notice this from the second to the third month of conception.
Implantation bleeding
It is one of the first symptoms of pregnancy, although it does not happen in all women. Implantation bleeding occurs about 12 days after ovulation, on the days when menstruation is expected. This bleeding is distinguished by being short-lived - no more than 5 days - and very light. Implantation bleeding occurs because the blastocyst settles in the uterus and sometimes some veins that affect the endometrium break and cause bleeding.
Fatigue
Another sign of suspicion of pregnancy is fatigue, characterized by asthenia, weakness, and drowsiness. Although some women feel renewed energy, most would confess to intense fatigue. Some claim to fall asleep at any time of the day, sometimes shortly after getting out of bed, and others claim to feel so drowsy after dinner. Others feel pronounced fatigue at night. Such fatigue is often uncontrollable and requires sleep. An explanation for this strange desire to sleep has never been found. It is a frequent symptom in the first months of pregnancy and it is believed to be an effect of the high production of progesterone. This hormone is a sedative for humans, with strong tranquilizing and hypnotic effects. Another type of fatigue due simply to bodily exhaustion occurs in the later stages, but rarely occurs in the first trimester of pregnancy.
Interruption of menstruation
Two weeks after fertilization, the absence of menstruation will be noted. The cessation of menstruation in a healthy, sexually active woman of reproductive age, who has previously had a regular and predictable menstrual cycle, is a highly suggestive sign of pregnancy. It is a suspicious sign of pregnancy called amenorrhea and is not exclusive to pregnancy. In addition to pregnancy, causes of amenorrhea are physical illnesses (some of a certain severity, such as ovarian tumors, thyroid gland disorders, and many others), a very strong shock, anorexia, the effect of a plane trip, an operation, stress or anxiety can delay menstruation. The loss of menstruation during pregnancy also means that ovarian follicles do not mature during the 9 months that it lasts, so if a woman becomes pregnant on numerous occasions she could delay the age at which she has menopause.
Occasionally, after conception, one or two episodes of uterine bleeding are observed that simulate menstruation and are confused with it. It is called the Long-Evans sign and is more common in multiparous women than in primiparous women.
Likes
Change in taste and preference for certain foods may be one of the first signs. It is common to reject certain foods, drinks and odors such as cigarette smoke. A metallic taste in the mouth is often described, which changes the taste for food. Cravings are believed to be due to increased hormone levels; they are sometimes experienced in the second half of the menstrual cycle for the same reason. It is not convenient to satisfy cravings with foods of high caloric content, whose nutritional value is low.
Frequent urges to urinate
As the uterus expands, it presses on the bladder. Therefore, it tries to expel small amounts of urine, and many women have frequent urges to urinate from the first week after conception; they may need to go to the bathroom every hour. This is also due to the effect of progesterone, since it is a powerful relaxant of the smooth muscle, (which is the muscle from which the bladder, uterus and other organs are formed) which serves to keep the uterus at rest until delivery. time of delivery. Unless you feel burning or pain when you urinate, you don't need to see your doctor. By 12 weeks, the size of the uterus will increase so that it will rise up and out of the pelvic cavity. This will reduce the pressure on the bladder and the frequency of urination so the bladder falls to one side.
Breast Changes
Engorgement and turgidity occur in the breasts due to the hormonal factor and the appearance of colostrum. It can appear in early stages of pregnancy due to the increase in prolactin, among other hormones. The areolas become more sensitive and hyperpigmented.
Skin manifestations
There is hyperpigmentation of certain areas of the skin during pregnancy. Abdominal stretch marks and at the level of the breasts also appear in some pregnant women. In other women, the appearance of chloasma at the level of the skin of the face is noted. These hyperpigmentations can occur with the use of oral contraceptives and in collagen diseases, while stretch marks are also a sign in Cushing's syndrome.
Vaginal mucosa
As a consequence of the increase in the vascularization of the vagina and cervix during pregnancy due to the vascularizing effect of progesterone, it is noted that the mucosa of these structures turns purple. This bluish change of the vaginal mucosa and cervix is known as the Chadwick-Jacquemier sign.

Signs of probability
They are fundamentally characteristic signs and symptoms of pregnancy that provide a high level of probability to the diagnosis of pregnancy.
Hormonal determinations
The presence of the hormone human chorionic gonadotropin (hCG) in maternal plasma and its excretion in the urine are the basis of hormonal studies of pregnancy. Production of this hormone by the syncytiotrophoblast begins very early in pregnancy. Sensitive tests can detect the hCG hormone in maternal plasma or urine 9 to 10 days after ovulation. This hormone is the basis of most pregnancy tests, although they may use different techniques, such as radioimmunoassay., monoclonal antibodies, immunofluorescence, and home tests using the hemagglutination principle. Other hormones that increase with pregnancy include estrogens, especially estriol, and progesterone.
Abdominal size
Usually, by twelve weeks of gestation it becomes possible to palpate the uterus above the pubic symphysis or mons pubis. From that moment on, the uterus continues to gradually increase until the end of the pregnancy. The increase in abdominal size can also be due to other causes that exclude pregnancy, such as uterine fibroids, ovarian tumors, ascites, etc.
Shapes of the uterus
- Noble-Budin Sign
From eight weeks of gestation, the pressure of the gestational product causes the bottoms of the sac that form at the junction of the vagina with the sides of the cervix to be occupied. So it is perceived in the vaginal touch, the rounded and turgid shape of the uterus when exploring the deep sides of the cervix.
- Sign of Hegar
From the sixth to eighth week of pregnancy, during bimanual examination the uterus feels excessively soft, pasty, and elastic—especially the isthmus of the uterus—in contrast to the hard, firm cervix.
- Signo de Piskacek
When performing the physical examination of the uterus, especially if the implantation of the embryo occurred close to one of the orifices of the fallopian tubes, an asymmetry is perceived with prominence towards the uterine horn that supports the implantation. It is a sign which can also be seen with the use of oral contraceptives.
- Sign of Goodell
Related to changes in the cervix, which becomes soft with pregnancy as opposed to being hard in non-pregnancy states. The analogy is made to feeling the cervix as touching the buccal lips, rather than feeling it normally what it would be like to touch the tip of the nose.
Braxton Hicks contractions
After the 17th week of gestation, slight uterine contractions are perceived, hardening at times in order to facilitate better blood flow to the placenta, endometrium, and fetus. These contractions are characterized by the fact that they encompass the entire uterus, starting at the top and gradually working downward and tend to help the uterus grow. They differ from labor contractions in that they are usually painless and irregular.
Fetal Rally
During the second half of pregnancy, between the fourth and fifth month, fetal parts can be palpated through vaginal examination. When the examiner gently pushes the fornix surrounding the cervix, he can appreciate the separation of the fetus from his finger and the return of the finger to its initial position in contact with the examiner's finger. It is a sign that on rare occasions can be felt in bulky tumors of the ovary concomitant with ascites.
Fetal palpation
From about the fifth month of pregnancy it is possible for an experienced examiner to feel the fetal parts through the maternal abdominal wall, a maneuver that is most successful towards term. Similar parts can be palpable in intra-abdominal tumors, some subserosal fibroids can, for example, become the same size and consistency as the fetal head, causing diagnostic errors.
Signs of a certain pregnancy
The positive signs of certainty of a pregnancy consist of being able to demonstrate without error the presence of embryonic structures by means of ultrasound and other radiological images.
Fetal cardiac activity
Identifying separate and distinct fetal heartbeats from the mother's ensures the diagnosis of pregnancy. Fetal heart activity can be auscultated with a stethoscope or special fetoscope, or with Doppler ultrasound. The fetal heartbeat is fast (between 120 and 160 beats per minute), and can be accurately identified from the 19th and 20th week, except in obese women in whom it is difficult to hear the fetal focus.
Ultrasound scan
At any time during pregnancy, especially in the presence of a mature fetus in the second half of pregnancy, both its anatomical parts and the yolk sac can be demonstrated by two-dimensional or three-dimensional transabdominal ultrasound.
Risk factors
There are pregnancies that, due to their special circumstances, require specific care and monitoring. Unforeseen complications or problems can arise in them that must be attended to promptly and professionally to avoid placing the mother or baby at risk. Some of these risk factors are listed below.
Malnutrition
A woman's nutrition before, during and after pregnancy is fundamental to having healthy children. Nutrient requirements increase considerably during pregnancy and lactation. A woman who arrives malnourished or becomes malnourished during pregnancy may have complications during pregnancy and delivery. As well as possibilities of having a low birth weight child (less than 2500 g). These children are more likely to:
- grow and develop with delay.
- contract infections and die (the risk increases the lower the weight of the birth).
- have low micronutrient reserves, which can lead to diseases such as anemia, Zinc deficiency or vitamin A, etc.
- risk developing heart disease, hypertension, obesity and adult diabetes.
- cause malformations during fetal development, such as a poor closure of the neural tube, which causes spina bifida disease.
It is very important for women to consume folic acid (vitamin B9), to avoid malformations in the fetus such as Spina bifida. In addition, it is also positive to consume all kinds of essential fatty acids (omega 3 fatty acid, omega 6 fatty acid) that contribute to a good development of the nervous system, since the myelin sheaths are made up of these fats that we can only obtain through diet., and the fetus, solely through maternal feeding.
It is also important not to eat raw foods such as Serrano ham, sushi, etc... since they may contain microorganisms that cause an infection that can affect the fetus and endanger its life.
Adolescence
40% of women in developing countries give birth before their 20th birthday. Very few of these pregnancies are planned or desired by adolescents. Many of them are forced by social pressures to have early marriages and early pregnancies, or are the result of adolescents denied free access to contraceptives. Adolescent pregnancy can have both short-term and long-term adverse health consequences. In the short term the outcome of the pregnancy will most likely be unfavorable. One reason is biomedical: the pregnant adolescent girl is more prone to toxemia of pregnancy and cephalopelvic disproportion when the pelvic bones have not fully developed. and she is more likely to have a low birth weight baby. Another type of long-term consequences are obstetric fistulas, which as a result of prolonged or obstructed labor, is a hole between the vagina and the bladder or rectum, which causes the woman to suffer from chronic incontinence. This condition affects more than two million girls and women worldwide and it is estimated that between 50,000 and 100,000 new cases are added each year.
Pregnant adolescents are more likely to be malnourished and give birth to underweight children. For physical and social reasons:
- their bodies are not yet fully developed, so their nutrient needs are very high during pregnancy. They also have greater chances of dying during pregnancy or breastfeeding than older women. This is mainly due to the level of poverty in which they live, which not only exposes the mother to children. It is noted that the situation of pregnant women was presented as complex and difficult before, during and after birth, this because of economic deficiencies. Poverty leads to lower educational opportunities, education that would reduce pregnancies at an early age and thus poverty. This is because if the pregnancy occurs in conditions of poverty it will surely have economic and social conditions. Intergenerational repetition of teenage pregnancy can be an intermediary mechanism in the intergenerational reproduction of poverty.
- Some girls are afraid to say they are pregnant, and for this reason they delay prenatal care. Some girls are forced to leave school and in some cases their home, so they must seek livelihood for themselves, and in some cases they resort to prostitution to achieve it.
These dangers can be addressed by warning girls and adolescents about the risks of pregnancy and explaining the different contraceptive methods. In addition, they should be observed and counseled if they are pregnant.
Anemia
Maternal anemia is a major risk factor and can affect pregnancy, especially during the first trimester. It can cause low birth weight in the baby. To prevent these risks, it is necessary to take all the necessary measures to diagnose and correct the anemia of the mother.
Women often make the mistake of attributing the presence of anemia to menstrual bleeding and limiting themselves to prescribing iron supplements, without carrying out the necessary evaluations to find or rule out possible diseases that cause anemia. The main Causes of anemia include low iron intake, excessive losses (alterations in the menstrual cycle, intestinal microbleeding), or processes that occur with chronic intestinal inflammation or alterations in intestinal absorption, such as celiac disease and undiagnosed non-celiac gluten sensitivity. nor treat (anemia may be its only manifestation, in the absence of digestive symptoms), or Crohn's disease.
Undiagnosed Celiac Disease
Undiagnosed and untreated celiac disease is a relatively common but poorly understood cause of a variety of reproductive disorders. It is an autoimmune disease caused by the consumption of gluten, which can affect any organ. It usually presents without any digestive symptoms and most cases go unrecognized and undiagnosed. Reproductive disorders are often the only indication of the presence of celiac disease, such as irregular periods, infertility or reduced fertility, miscarriage, complications during pregnancy, intrauterine growth restriction, stillbirth, premature delivery, low birth weight and lactation disorders.
In general, a strict gluten-free diet prevents or decreases the risk of reproductive disorders.
Pregnancy complications or failures cannot be explained simply by malabsorption, but by the autoimmune response caused by gluten exposure, which causes damage to the placenta.
In addition, pregnancy can be a trigger for the development of celiac disease in women with a genetic predisposition who consume gluten.
Antepartum hemorrhage
Before 24 weeks, vaginal bleeding can lead to miscarriage. Afterwards, the fetus is considered viable, that is, it could survive outside the mother's womb. Bleeding after 24 weeks is known as antepartum hemorrhage, and the two main causes come from the placenta.
Abruption of the placenta
If the placenta detaches from the uterus, bleeding will occur. The blood accumulates until it spills out of the cervix, and is accompanied by intense pain and uterine contractions. It is considered an obstetric emergency, since it endangers the life of both the mother and the fetus and only in very special cases does it not end in an emergency caesarean section.
Planta previa
When the placenta is attached to the lower wall of the uterus, it is called placenta previa. If it lies wholly or partly on the cervix, it can be dangerous during childbirth, causing bleeding and interrupting the blood circulation of the fetus. The problem is detected with ultrasound. If bleeding occurs, she will be admitted to the hospital and the child will be delivered by caesarean section.
Diabetes
If the pregnant woman has diabetes mellitus, she should make sure that her situation is under control before becoming pregnant, so that the chances of having a healthy child and a normal delivery are as high as possible. It is likely that you will need a greater amount of insulin during pregnancy, for which a strict medical follow-up must be carried out, for the monitoring of fetal well-being, monitoring of glycemia levels and dietary management.
Some women are diagnosed with gestational diabetes mellitus, a type of diabetes that develops only during pregnancy and usually disappears soon after delivery. The risks of this type of diabetes are minor and insulin is rarely required; reducing sugar intake is usually enough. The main complication in the children of mothers with gestational diabetes is fetal macrosomia (children weighing more than 4 kilos).
A 2018 review concludes that one of the main risk factors for developing both type 1 and type 2 diabetes is gluten consumption. This, present in wheat, rye, barley and oats, causes increased intestinal permeability, regardless of genetic predisposition, that is, both in celiac and non-celiac patients. Gluten contains cytotoxic peptides that cross the intestinal barrier and cause systemic inflammation. These peptides penetrate the pancreas, affect its morphology, and can induce stress on beta cells, which are responsible for synthesizing and secreting insulin. Animal studies and one human study have shown that a gluten-free diet during pregnancy reduces the risk of the baby developing type 1 diabetes; there is a change in the morphology of the pancreas, including an increased number of pancreatic islets.
Ectopic Pregnancy
An ectopic pregnancy develops outside the uterus, usually in one of the fallopian tubes, but it can also be in the ovaries, cervix, or intra-abdominal organs. It can cause abdominal pain due to the growth of the embryo in the tube or due to internal abdominal bleeding. Unfortunately, it is difficult to diagnose an ectopic pregnancy and there are still women who die as a result. There are a series of conditions that favor the increased risk of suffering from ectopic pregnancies. These included a prior history of pelvic infection, use of a contraceptive intrauterine device (but not the Mirena coil), and a prior ectopic pregnancy. Women who meet any of the aforementioned conditions are immediately checked at a maternity center to ensure that the development of the pregnancy is normal. Ectopic pregnancy must be treated by surgery or with a drug. The operations consist of laparoscopic or open surgery, depending on the circumstances and conditions of the mother, and usually involve the removal of the affected tube. They usually cause reduced fertility.
Heart Disease
Most women with heart problems have a stable pregnancy, although sometimes they must resort to antibiotics to protect their arteries when giving birth. If you have any significant heart disease, the cardiologist will take care of notifying you. Women with pacemakers, a heart transplant and other coronary surgery can carry a safe and normal pregnancy. Those with muscle abnormalities should consult it before becoming pregnant.[citation needed]
Hypertension
Gestational hypertension, is the appearance of hypertension above 140/90 mmHg, in a pregnant woman without a previous diagnosis, after 20 weeks of pregnancy. If there is hypertension prior to pregnancy, it requires medical check-up and treatment before pregnancy. gestation. Possibly requires change of drugs and monitoring of renal function. With adequate follow-up, it is possible to have a normal pregnancy and delivery. If you develop gestational hypertension during pregnancy, you may require outpatient or hospital treatment, depending on the severity. Sometimes it is necessary to advance delivery, by induction or caesarean section, to prevent complications for the mother and the fetus. An increase in blood pressure from the 20th week of pregnancy can be a symptom of preeclampsia, a condition that potentially threatens the life of the pregnant woman and the newborn.
Important information
- Between 18 and 20 weeks the perception of fetal movements begins.
- In the 38th week of pregnancy the doctor will be able to diagnose pelvic narrowing.
- In week 20 the fetal heart will have a heart rate of between 110-160 ppm which will be perceived through stethoscope.
Physiological changes during pregnancy
The pregnant woman is in a chronic hypervolemic state. Total body water volume is increased due to increased salt and water retention by the kidneys. This greater amount of water causes dilution of the blood, which would explain the physiological anemia of pregnancy that persists throughout the pregnancy.
Increased blood volume causes an increase in cardiac output, urinary volume, and maternal weight. The action of certain prostaglandins causes bronchodilation and increased respiratory rate. At the renal level, a slight decrease in creatinine clearance and other metabolites is seen.
The weight of the mother during pregnancy increases at the expense of the weight of the fetus, the weight of amniotic fluid, placenta and ovular membranes, the increase in the size of the uterus, the retention of maternal fluids and the inevitable deposition of fat in tissues maternal. The mother's metabolism also increases during pregnancy.
Heart rate increases to an average of 90 beats per minute. Blood pressure remains constant or often slightly decreased. Venous resistance increases, especially below the pregnant waist. The heart tends to enlarge, a condition called especially left ventricular hypertrophy, and it disappears within a few weeks after delivery. The circulating presence of prostaglandins causes vasodilation in opposition to the physiologic vasoconstrictors angiotensin and norepinephrine, especially since angiotensin II is increased to maintain normal blood pressure. Hypertension and the appearance of edema are usually warning signs in pregnancy.
The glomerular filtration rate or index and kidney perfusion increase at the expense of increased cardiac output and renal vasodilation. This causes a slight increase in blood creatinine values due to a decrease in creatinine clearance and also in urea nitrogen. The decrease in the partial pressure of carbon dioxide in the maternal blood causes an increase in the renal excretion of bicarbonate.
Prenatal human development
Prenatal development after fertilization month by month:
Month 1: Measure 4 mm and weigh 1 g. Incipient development of the head. The heart is already beating

Month 2: Measure 3 cm and weigh 3 g. Development of arms and legs, as well as the brain and internal organs.

Month 3: Measure 10 cm and weigh 45 g. Development of the eyelids and movement of the limbs

Month 4: Measure 15 cm and weigh 180 g. It's covered with lanugo. The intestine begins to be filled with meconium. The skin is still very thin, almost transparent.

Month 5: Measure 18 cm and weigh 500 g. It grows hair from the head, eyelashes and eyebrows. Development of the immune system

Month 6: Measure 25 cm and weigh 1000 g. The face is completely formed. The skin is covered by a fatty material called homey vernix. Open your eyes and move a lot.
Month 7: Measure 30 cm and weigh 1500 g. They start moving their lungs. It increases subcutaneous fat and no longer fits well in the uterus.

Month 8: Measure 35 cm and weigh 2500 g. The skin is usually put to the bottom (zephalic position) The skin is thickened, acquiring the definite thread tone.
Month 9: It measures 50 cm and weighs approximately 3000 g. The lungs are already fully formed for outer life. Lanugo falls and the skin is stretched.










7-week ultrasound

12-week ultrasound

13-week ultrasound

13-week ultrasound

17-week ultrasound

17-week ultrasound

20-week ultrasound







Epigenetics of pregnancy
Life habits and the maternal environment play a fundamental role in the correct development of the embryo, both at an early age and, in some cases, in adulthood. Some habits such as tobacco or alcohol consumption cause mutations in the child, increasing the risk factor for certain diseases. In addition to mutations, epigenetic changes occur. They are certainly heritable reversible DNA alterations produced by the environment. The most studied factors are: nutrition, diabetes, depression or stress.
Folic Acid
Many studies have shown that a diet rich in folic acid during pregnancy prevents neural tube defects, decreased intrauterine growth, autism spectrum disorder, congenital heart defects, allergies, and cancer. During pregnancy, the availability of methyl donors from dietary sources can alter S-adenosyl-methionine synthesis and thus alter DNA methylation and histone modifications in the fetal epigenome.
In a mouse model, it was shown that supplementation with methyl donors before and during pregnancy induced a gain in methylation and, therefore, changes in the phenotype and longevity of the offspring. The offspring of mice with a folic acid deficiency presented changes in the brain epigenome and decreased body weight.
High-fat diet
Like methyl donors, a high-fat maternal diet has been shown to induce alterations in the methylation pattern, increasing insulin sensitivity and offspring body weight. A study of the offspring of women with pregestational diabetes or GDM has shown that aberrant maternal metabolism is associated with poorer intellectual performance and psychomotor development. In addition, methylation changes were observed in offspring on high-calorie diets. DNA methylation was reduced in the promoter of the transcription factor Zfp423. This deregulation of Zfp423 may enhance differentiation into adipose tissue during fetal development and alter metabolic function.
Malnutrition
Moderate maternal malnutrition produced alterations in the level of methylation and acetylation of the genes related to the fetal hypothalamic pathways. Such changes were associated with reduced DNMT activity. Human studies have shown an increased risk of death, spina bifida, and schizophrenia in offspring. Among other causes, people exposed to famine have hypomethylation of the IGF2 gene, related to fetal growth.
Stress and depression
Maternal stress and depression have been linked to a four-fold increase in the risk of developing depression in the child, in addition to increasing the risk of adult-onset illnesses. An epidemiological study has also suggested that there is a strong correlation between maternal stressors and birth weight. Stress-induced fetal corticosterone exposure is one of the main causes of this correlation.
At the epigenetic level, a mouse model demonstrated that prenatal stress decreases BDNF expression in the amygdala and hippocampus both at weaning and in adulthood.
Transsexual pregnancy

A transsexual male who retains female genitalia can resume the ovulatory cycle upon discontinuation of androgen therapy, thereby maintaining reproductive capacity, including pregnancy. This has been the case of Thomas Beatie, a transsexual male (born female) who between 2008 and 2010 gave birth to three children.
Contenido relacionado
Arundinella
Antinoria
Agrostis